
Page 10 - Carotid and peripheral vascular interventions textbook
P. 10
CAROTID AND PERIPHERAL VASCULAR INTERVENTIONS: STEP-BY-STEP
After f nishing DSA, the catheter is torqued towards familiar with less subsequent vascular complications.
the ostial contralateral iliac artery, the Glidewire is then This approach also permits to treat contralateral common
®
forwarded distally to the CFA level enabling suitable length to femoral and ostial SFA disease. The disadvantages of this
forward a selective catheter within the distal external iliac approach are less catheter and wire support and trackability
artery. In diff cult anatomy, roadmap function with f uoroscopy as it is working from a distance, technical diff culty with
may be used to facilitate during the Glidewire navigation. calcif ed and/or angulated aortoiliac bifurcations, and not
®
As compared to antegrade common femoral approach, feasible with previous aorto-bifemoral bypass or aortoiliac
this retrograde access is much easier to achieve, more kissing stents.
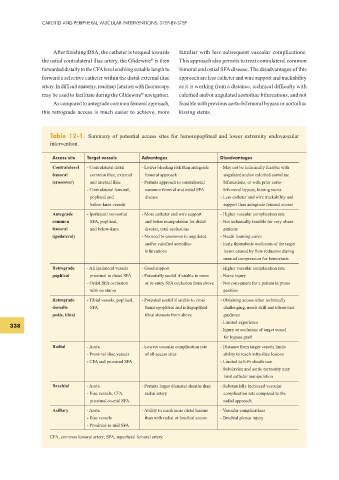
Table 12-1. Summary of potential access sites for femoropopliteal and lower extremity endovascular
intervention.
Access site Target vessels Advantages Disadvantages
Contralateral - Contralateral distal - Lower bleeding risk than antegrade - May not be technically feasible with
femoral common iliac, external femoral approach angulated and/or calcif ed aortoiliac
(crossover) and internal iliac - Permits approach to contralateral bifurcations, or with prior aorto-
- Contralateral femoral, common femoral and ostial SFA bifemoral bypass, kissing stents
popliteal and disease - Less catheter and wire trackability and
below-knee vessels support than antegrade femoral access
Antegrade - Ipsilateral non-ostial - More catheter and wire support - Higher vascular complication rate
common SFA, popliteal, and better manipulation for distal - Not technically feasible for very obese
femoral and below-knee disease, total occlusions patients
(ipsilateral) - No need to crossover in angulated - Needs learning curve
and/or calcif ed aortoiliac - Early thrombotic occlusion of the target
bifurcations lesion caused by f ow reduction during
manual compression for hemostasis
Retrograde - All ipsilateral vessels - Good support - Higher vascular complication rate
popliteal proximal to distal SFA - Potentially useful if unable to cross - Nerve injury
- Ostial SFA occlusion or re-entry SFA occlusion from above - Not convenient for a patient in prone
with no stump position
Retrograde - Tibial vessels, popliteal, - Potential useful if unable to cross - Obtaining access often technically
dorsalis SFA femoropopliteal and infrapopliteal challenging, needs skill and ultrasound
pedis, tibial tibial stenosis from above guidance
- Limited experience
338
- Injury or occlusion of target vessel
for bypass graft
Radial - Aorta - Lowest vascular complication rate - Distance from target vessels limits
- Proximal iliac vessels of all access sites ability to reach infra-iliac lesions
- CFA and proximal SFA - Limited to 6-Fr sheath size
- Subclavian and aortic tortuosity may
limit catheter manipulation
Brachial - Aorta - Permits larger diameter sheaths than - Substantially increased vascular
- Iliac vessels, CFA, radial artery complication rate compared to the
proximal-to-mid SFA radial approach
Axillary - Aorta - Ability to reach more distal lesions - Vascular complications
- Iliac vessels than with radial or brachial access - Brachial plexus injury
- Proximal-to-mid SFA
CFA, common femoral artery; SFA, superf cial femoral artery.