
Page 6 - Carotid and peripheral vascular interventions textbook
P. 6
CAROTID AND PERIPHERAL VASCULAR INTERVENTIONS: STEP-BY-STEP
A B
!
#
"
!"#
!$#
!%#
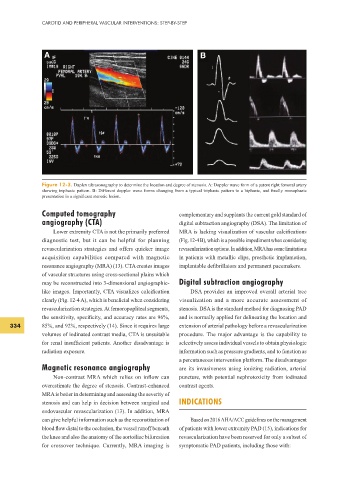
Figure 12-3. Duplex ultrasonography to determine the location and degree of stenosis. A: Doppler wave form of a patent right femoral artery
showing triphasic pattern. B: Different doppler wave forms changing from a typical triphasic pattern to a biphasic, and f nally monophasic
presentation in a signif cant stenotic lesion.
Computed tomography complementary and supplants the current gold standard of
angiography (CTA) digital subtraction angiography (DSA). The limitation of
Lower extremity CTA is not the primarily preferred MRA is lacking visualization of vascular calcif cations
diagnostic test, but it can be helpful for planning (Fig. 12-4 B), which is a possible impediment when considering
revascularization strategies and offers quicker image revascularization options. In addition, MRA has some limitations
acquisition capabilities compared with magnetic in patients with metallic clips, prosthetic implantation,
resonance angiography (MRA) (13). CTA creates images implantable def brillators and permanent pacemakers.
of vascular structures using cross-sectional plains which
may be reconstructed into 3-dimensional angiographic- Digital subtraction angiography
like images. Importantly, CTA visualizes calcif cation DSA provides an improved overall arterial tree
clearly (Fig. 12-4 A), which is benef cial when considering visualization and a more accurate assessment of
revascularization strategies. At femoropopliteal segments, stenosis. DSA is the standard method for diagnosing PAD
the sensitivity, specif city, and accuracy rates are 96%, and is normally applied for delineating the location and
334 85%, and 92%, respectively (14). Since it requires large extension of arterial pathology before a revascularization
volumes of iodinated contrast media, CTA is unsuitable procedure. The major advantage is the capability to
for renal insuff cient patients. Another disadvantage is selectively assess individual vessels to obtain physiologic
radiation exposure. information such as pressure gradients, and to function as
a percutaneous intervention platform. The disadvantages
Magnetic resonance angiography are its invasiveness using ionizing radiation, arterial
Non-contrast MRA which relies on inf ow can puncture, with potential nephrotoxicity from iodinated
overestimate the degree of stenosis. Contrast-enhanced contrast agents.
MRA is better in determining and assessing the severity of
stenosis and can help in decision between surgical and INDICATIONS
endovascular revascularization (13). In addition, MRA
can give helpful information such as the reconstitution of Based on 2016 AHA/ACC guidelines on the management
blood f ow distal to the occlusion, the vessel runoff beneath of patients with lower extremity PAD (15), indications for
the knee and also the anatomy of the aortoiliac bifurcation revascularization have been reserved for only a subset of
for crossover technique. Currently, MRA imaging is symptomatic PAD patients, including those with: